

講義といってもコロナの影響でWEB形式になっています。ご覧のように複十字病院でもWEB会議などが出来る体制ができたため、田中先生は会議室に籠って講義をしています。たま北部医療センターと当院は連携が強く、初期研修医、後期研修医の先生が呼吸器科ローテーションのために複十字病院で研修をうけています。みなさん熱心なので当院のベテラン医師たちにも活気が出ます。
田中先生は呼吸困難についていつも通りの切れの良い講義をしていますが、相手が見えないので少しさみしそうです笑。
呼吸困難とは「呼吸の不快な自覚」
講義といってもコロナの影響でWEB形式になっています。ご覧のように複十字病院でもWEB会議などが出来る体制ができたため、田中先生は会議室に籠って講義をしています。たま北部医療センターと当院は連携が強く、初期研修医、後期研修医の先生が呼吸器科ローテーションのために複十字病院で研修をうけています。みなさん熱心なので当院のベテラン医師たちにも活気が出ます。
田中先生は呼吸困難についていつも通りの切れの良い講義をしていますが、相手が見えないので少しさみしそうです笑。
呼吸困難とは「呼吸の不快な自覚」

久しぶりに病理カンファレンスが行われました。呼吸器科の醍醐味の一つは病理カンファレンスで1例を掘り下げてディスカッションすることです。当院には、放射線科には黒崎敦子先生、病理では岡輝明先生と武村民子先生がいらっしゃり、とても贅沢な環境でカンファレンスを行うことができます。会は臨床の田中先生がリードして進められます。他施設も加わるMDDの会は中断のままですが、一足先に病理カンファレンスが出来てとても充実した時間となりました。
本日は3例を検討し、VATS生検の2例は間質性肺炎でした。なんとどちらも、画像、病理像は異なるANCA陽性間質性肺炎でした。残り1例はTBLBで画像、病理所見とも過敏性肺炎様の薬剤性肺傷害でした。
個人的には1例目はしっくりくる、アクティブな間質性肺炎例でしたが2例目はPPFE様の病理像も伴っており、ANCA関連といっても病態は異なる印象を受けました。びまん班でもメインテーマの一つとなっており、診断、治療法など新たな展開を期待したいです。
新ガイドラインには当院が著者に加わった論文が8つありました。3つは外科からになります。最近当院も含め外科治療に関する論文が日本から3つ報告されていてどれも興味深いです。写真は当院外科センター長の白石先生です(以前ブログで紹介した写真です)。

18. Morimoto K, Namkoong H, Hasegawa N, et al; Nontuberculous Mycobacteriosis Japan Research Consortium. Macrolide-resistant Mycobacterium avium complex lung disease: analysis of 102 consecutive cases. Ann Am Thorac Soc 2016; 13:1904–11
20. Griffith DE, Eagle G, Thomson R, et al; CONVERT Study Group. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT). a prospective, open-label, randomized study. Am J Respir Crit Care Med 2018; 198:1559–69.
136. Kadota JI, Kurashima A, Suzuki K. The clinical efficacy of a clarithromycin-based regimen for Mycobacterium avium complex disease: a nationwide post-marketing study. J Infect Chemother 2017; 23:293–3
170. van Ingen J, Aksamit T, Andrejak C, et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: an NTM-NET consensus statement. Eur Respir J 2018; 51:1800170.
202. Namkoong H, Morimoto K, Nishimura T, et al. Clinical efficacy and safety of multidrug therapy including thrice weekly intravenous amikacin administration for Mycobacterium abscessus pulmonary disease in outpatient settings: a case series. BMC Infect Dis 2016; 16:396.
218. Shiraishi Y, Fukushima K, Komatsu H, Kurashima A. Early pulmonary resection for localized Mycobacterium avium complex disease. Ann Thorac Surg 1998; 66:183–6.
219. Shiraishi Y, Nakajima Y, Katsuragi N, Kurai M, Takahashi N. Pneumonectomy for nontuberculous mycobacterial infections. Ann Thorac Surg 2004; 78:399–403.
220. Shiraishi Y, Nakajima Y, Takasuna K, Hanaoka T, Katsuragi N, Konno H. Surgery for Mycobacterium avium complex lung disease in the clarithromycin era. Eur J Cardiothorac Surg 2002; 21:314–8.
ガイドラインのMethodに下記の記載があります。A medical librarian (S.K.) designed a search strategy using medical subject heading keywords and text words (see online supplement) limited to human studies and articles with English abstracts. Databases searched included MEDLINE, EMBASE, Cochrane Registry of Controlled Trials, Health Technology Assessment, and the Database of Abstracts of Reviews of Effects from 1946 through July 2015. An update was performed in May 2016 prior to the final meeting at the ATS International Conference and a final update was performed in June 2018 prior to manuscript submission. つまり、本来は2016年のアップデートでガイドラインPublishまで行きたかったところを時間がかかって2018年アップデートが加えられたということだと思います。ガイドライン作りは大変ですね。
その他、日本発のデータが複数引用されています。束村先生の診断、Miwa先生の2剤治療、田中先生のマクロライドベース治療は光っていますね。
非英語論文でも各国の論文の英語アブストラクトはチェックしていたようで、日本からのデータについて20本ほど内容確認を受けました。
「2.肺M. kansasii症患者では、経験的治療よりもリファンピシンの感受性結果に基づいて治療を行うことを支持する(条件付き推奨)」
感受性試験に関する推奨の続きです。
コメント
肺非結核性抗酸菌症化学療法に関する見解―2012年改訂では下記の記載になっています。 「わが国での RFP耐性肺カンサシ症の割合は1%未満と 少なく,特に初回治療例ではほとんどない19)。従って全 例に薬剤感受性検査を実施する必要はなく,再発例もし くは標準療法で治療効果の乏しい場合にのみ結核菌用の 薬剤感受性検査を実施する。」
複十字病院のM. kansasii症をまとめた報告でも、耐性株は認められなかったこと、再発率も低いことから当院でも診断時の感受性は行っていません。肺Mycobacterium kansasii症の臨床・分子生物学的検討. Kekkaku Vol. 90, No. 4 : 453_456, 2015
「3.肺M. xenopi症患者では、薬剤感受性結果に基づく治療を推奨あるいは反対するにはエビデンスが不足している。」
コメント
2007ステートメントは、MAC, M. kansasii, MABCを中心としたものでしたが、新ガイドラインではM. xenopiがガイドラインに加わりました。M. xenopiが多い地域(フランスおよびカナダ(オンタリオ))からそれぞれガイドラインメンバーに加わっているのも影響しているかもしれません。
・診断法はこれまでと変わらないと先日記載しましたが、新しいガイドラインでは菌種についてMAC, M. kansasii, MABCに制限しなくなっていますね。病原性の低いM. gordonaeと強いM. kansasiiを挙げ、さらに病原性も地域差があることを示唆して柔軟に判断するように記載しています。
・個人的見解ですが、M. gordonaeの診断基準については新たな菌の基準を提案しています。Clinical and microbiological features of definite Mycobacterium gordonae pulmonary disease: the establishment of diagnostic criteria for low-virulence mycobacteria. Morimoto K, Kazumi Y, Shiraishi Y, et al.Trans R Soc Trop Med Hyg. 2015 Sep;109(9):589-93. doi: 10.1093/trstmh/trv058. Epub 2015 Jul 25.
・また、日本では稀な菌ですが、DDHで診断されていた中にはM. heckeshornenseがM. xenopiと誤同定されていることも報告しており、今後質量分析で診断された症例データの蓄積が必要と思っています。Mycobacterium heckeshornense lung infection that was diagnosed as Mycobacterium xenopi disease by DNA-DNA hybridization (DDH). K Morimoto 1, Yuko Kazumi, Shinji Maeda, et al.Intern Med. 2011;50(11):1251-3. doi: 10.2169/internalmedicine.50.4628. Epub 2011 Jun 1.
「4.肺M. abscessus症患者では、経験的治療よりもマクロライドおよびアミカシンの感受性結果に基づいて治療を行うことを支持する(条件付き推奨)。マクロライドに対しては、潜在的マクロライド耐性について評価するため、14日間の培養・erm(41)遺伝子のシークエンスが必要である。」

コメント
・質量分析を使ってもM. abscessus complexの亜種同定はできません(研究レベルでは少し報告があります)。現在国内外で他の手法による研究が盛んになっており、近い将来亜種分離が容易にできることが期待されます。当院ではmultiplex PCR法でルーチンで亜種分離しています(J Clin Microbiol. 2014 Jan;52(1):251-9. doi: 10.1128/JCM.01327-13.)。
・感受性検査を結核用の感受性検査や遅速発育菌(MAC含む)用のBrothMIC NTM®で行っていないでしょうか。セットオーダーを多用する検査会社側の問題もありますが、依頼する側で修正しないといけません。M. abscessus complex含む迅速発育菌の感受性検査にはBrothMIC RGM®(極東)で依頼しましょう。
当科ではびまんカンファレンスという、びまん性肺疾患に特化したカンファレンスを行っており、そこで紹介された論文になります。院内で定期に行われているカンファレンスにはその他:呼吸器カンファレンス、キャンサーボード、病理カンファレンス、MACカンファレンス、気管支鏡カンファレンス、があります。
INBUILDおよびINPULSIS試験のデータを使用して、進行性線維化を伴う間質性肺疾患(PF-ILD)の自然経過を調査した。
2つのINPULSIS試験の対象者は特発性肺線維症(IPF)の臨床診断を受け、INBUILD試験の対象者はIPF以外のPF-ILDを有し、2年以上のマネージメントにもかかわらずILD進行のプロトコルの基準を満たした。プラセボ群のデータを使用して、INBUILD試験の52週間での努力肺活量(FVC)の低下率(mL・year-1)と死亡率を、INPULSIS試験の統合データと比較した。
INBUILD試験(n = 331)におけるFVCの調整済み平均年間低下率は、INPULSIS試験(n = 423)で観察されたものと同様であった(それぞれ、-192.9 mL・year-1および-221.0 mL・year-1) ;名目p値= 0.19)。 52週目に%FVCが10%以上低下した被験者の割合は、INBUILD試験で48.9%、INPULSIS試験で48.7%であり、52週間で死亡した割合は、INBUILD試験で5.1%、INPULSIS試験で7.8%であった。%FVCの相対的な減少が10%を超えたものは、INBUILD試験(ハザード比3.64)およびINPULSIS試験(ハザード比3.95)での死亡リスクの増加と関連していた。
これらの調査結果は、マネージメントにもかかわらず進行しているIPF以外の線維化ILD患者は、未治療のIPF患者と同様の臨床経過が予想され、ILDが進行して早期死亡するリスクが高いことを示している。


2つのニンテダニブの臨床試験、INPULSIS (対象 IPF)のとINBUILD (対象 PF-ILD)のプラセボ群を比較した研究です。PF-ILDとIPFの予後は同等との結果ですが、INBUILD試験は対象者の60%以上がHRCTでUIP様の線維化パターンであることに注意が必要だと思います。Non-UIP線維化パターン例の予後がIPFと同様に悪いのかどうかはわかりません。
II: 肺NTM症は経験的(empirically)に治療すべきか、あるいはin vitroの薬剤感受性結果に基づいて治療すべきか?
1.肺MAC症患者では、経験的治療よりもマクロライドおよびアミカシンの感受性結果に基づいて治療を行うことを支持する(条件付き推奨)。

コメント:感受性試験と臨床効果の乖離は大きなテーマです。erm 遺伝子の存在はその一つを明らかにしたと言えます(耐性誘導が起こるため3日目感受性, 14日目耐性)。また、AMKについても進展(MICレベル、構成型遺伝子の特定)がありました。
・ガイドラインでは、cation-adjusted Mueller–Hinton brothでの感受性が推奨されていますが(CLSI推奨に基づく)、日本はBrothMIC NTM®を使っています。培地は異なりますがクラリスロマイシンの感受性を同キットで行うことは推奨の培地が入手困難な状況では許容されると考えます。実際にBrothMIC NTM®のクラリスロマイシンMIC分布を調べると(n=1516) 2峰性を示しており、耐性の判断には間違いはないと考えていますAnn Am Thorac Soc. 2017 Jan;14(1):49-56. doi: 10.1513/AnnalsATS.201607-573OC.。問題はアミカシン(AMK)です。AMK感受性試験で耐性の判断は≥64とされていますが、BrothMIC NTMではMIC16までしか測定できません。つまり16以上の菌株は耐性かもしれない、というところまでしか判断できません。リポソーマルAMKのRCTではAMK耐性例で陰性化を得た症例は無かったと報告されておりCAMと同様に耐性=無効となります。現在開発中のCLSIに準じた新しいSGM用のキットが早く使えるようなることを期待しています。
・クラリスロマイシン耐性は、23S rRNA(rrl)の変異であることは有名ですが、AMKの耐性は16S rRNAの変異(A1408G)であることが分かっています。
・(日本では)NTMが同定されても、結核の固形培地で感受性試験が行われているのをしばしば目にします。おそらく、トマツ、培養、感受性をセットにして依頼しているか、そのようなシステムがあるのだと思います。院内でそのような状態があるようでしたら、早急に止めるようにするべきと思います。
・BrothMIC NTMの結果を見て、エサンブトール(EB)耐性、レボフロキサシン(LVFX)感受性ゆえにCLA+LVFXを選択した、、というのは間違いです。EB抜きの治療はクラリスロマイシン耐性の原因となります。クラリスロマイシンとアミカシン以外の感受性結果は参考にしてはいけません。
・治療開始後に培養陽性が続くようであれば少なくとも6か月に1回は感受性検査を行いましょう。
・診断時クラリスロマイシン感受性検査を行うか否かは、初回耐性率によると思われ、議論になると思います。新ガイドラインでは初回検査を推奨しており、少なくとも気道感染やマクロライド療法投与などで暴露がある人は測定すべきと思います。
田中先生による初学者向けのシリーズです。私のびまん性肺疾患のイメージは、「男性医師」です(特にIPの話ですが)。画像や病理診断には女性の先生はいらっしゃいますが、残念ながら女子医師でIPを専門にしている方が少ない気がしています。入り口で苦手意識をもってしまうためでしょうか。是非初学者の方(勿論男性医師も)に楽しんで読んでほしいです~。

みなさん初めまして。みなさんは「びまん性肺疾患」「間質性肺炎」と聞くとなにを思い浮かべるでしょうか。
「疾患が細分化されすぎていて複雑でよくわからない!」
「専門としているひとは診断にこだわっているけれど、治療は同じでしょ。」
ごもっともな意見です。ぐうの音もでません。ですが、専門にしている人間にも言い分はあるんですよ。複雑系ほど面白い。治療も微妙に違うんです(微妙にね)。
このシリーズの目標は間質性肺炎をはじめとする びまん性肺疾患という高山を目の前にして立ちすくんでいるであろう、あなたのシェルパいや山岳ガイド、少なくとも道しるべ程度に山を登るお手伝いをすることです。立ちすくんでいなくても読むとなにかの足しになるかもしれません。10回読むとTポイントがたまるかも。では、一緒にびまん性肺疾患の山道に向かいましょう(昭和な文章はしかたない)。ちなみに私は根っからのインドア派で山登りが趣味ではないので間違っても実際の山登りに誘わないでください。
びまん性肺疾患とは?
両肺にびまん性に陰影がみられる疾患のことですから、多くは画像をもとに「これはびまん性肺疾患であるっ!」と分類されます。画像で両肺に広く変化がみられるものであれば原因は何でもありです。腫瘍も感染症も心原性肺水腫も含みます。びまん性肺疾患の専門家は全員、すべての疾患は びまんに通ず、びまんこそ最上位といいたいのですが、そこはグッとこらえて心のなかにしまっています(当社調べ)。
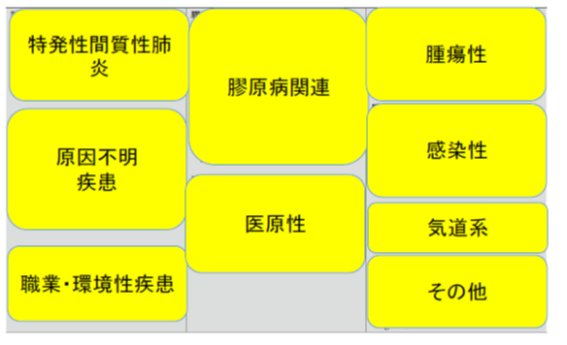
表 びまん性肺疾患
山脈(疾患のグループ)と個々の山々(疾患)。山多すぎ。
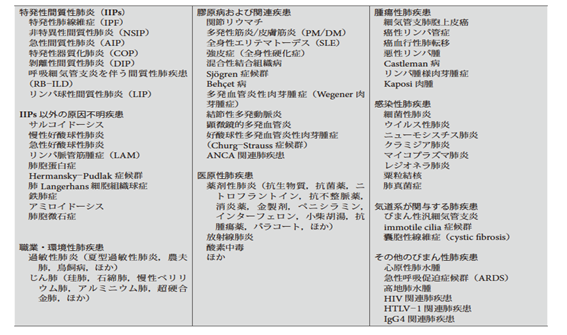
(日本呼吸器学会 特発性間質性肺炎診断と治療の手引き 改定第3版)
まず疾患のグループを眺めてみてはどうでしょうか。東の横綱が腫瘍性、西の横綱が特発性間質性肺炎です。わからないひとは「番付」で画像検索してください。

PICO-1の続きです。
とはいっても、空洞と塗抹だけで判断できないのが難しいところです。
以前にも紹介したnatural history(自然経過)のデータを示してhttps://wordpress.com/view/fukujuji.home.blog 安定しており、spontaneous sputum culture conversionが起こり得ること、若年、BMI良好、診断時塗抹陰性例はその予測因子となることを示しています(このデータを示すのは意外でしたが)。
そして、治療開始の判断は、空洞、塗抹陽性、菌種といった臨床所見に加えて、合併症、薬剤忍容性を踏まえて総合的に判断するように記載されています。
関係ない話ですが、、補足)
[年齢について]。 難しいのがガイドラインには記載されていませんが年齢の要素です。70歳、75歳、80歳、85歳、何歳が化学療法を避けるべき年齢でしょうか。一概には決められない問題だと思います。75歳で診断されて(小空洞あり)、無治療の方針がとられた患者さんが80歳で荒蕪肺となり強い症状をコントロールが出来なくなってしまうことも起こり得ます。患者背景を絞ったデータが乏しく判断が難しいのも確かですが、高齢の方には、個々の治療目標設定を進行抑制(陰性化は目指さず、空洞化や気管支拡張の進展を遅らせるなど)にして投与量を調節するなど、特に個別化が重要なのではないかと思います。
[治療アウトカムについて]。菌陰性化ではなくpatient oriented outcomes(PRO)で判断しようという動きがあるのは確かで、様々議論されている段階だと思います。しかし、たとえば臨床所見を考慮せず、治療の大変さ、副作用を心配する患者さんに、薬はやらなくていいですよ、と言えばその時のQOLは満足されますが長期的にはどうなのでしょうか。ある先生が「私は治療しなくても会話だけで患者QOLを改善させる事ができてしまう。QOL評価のみでNTM診療を行うのはリスクがある」と言っていました。今後のデータ集積が望まれます。

新しいNTMガイドライン(ATS/ERS/ECSMID/IDSA)については倉原先生が既にアップされているので概要は把握されていると思いますhttps://pulmonary.exblog.jp/29085698/。ここでは少しコメントを添える形にしたいと思います。
今回のガイドラインではERS, ECSMIDが加わっています。22の PICOquestionsが挙げられ、GRADEシステムで作成されたはじめてのNTM Guidelineになります。1997年、2007年はテキサスのWallace, Griffithらが驚くべき力で作成されていましたが、今回からデンバーのCharles Daley やオレゴンのKevin Winthropらが中心になっています(余談ですが米国はNTM症を呼吸器科と感染症科が半分ずつくらいで診ているのですよね。日本は90%以上が呼吸器科だと思います)。諸事情で遅れたことは理解していますが、随分かかりました。内容としてはM. abscessus complexの変化が一番大きいですが、MACについても我々は内容(違い)をしっかりと確認しておく必要があります。
「I: 肺NTM症は抗菌薬で治療すべきか、それとも進行のエビデンスをみるために注意深く追跡(Watchful waiting)すべきか?
1.肺NTM症の診断基準に合致する患者に対して、特に抗酸菌性塗抹(and/or)空洞がある患者においては、注意深い観察よりも治療開始を推奨する(条件付き推奨)。」
この第一のPICOの前には診断について記載されており、診断基準に変化が無かったことがわかります。また、次の文章がその最後に添えられています「Importantly, just because a patient meets diagnostic criteria for NTM pulmonary disease does not necessarily mean antibiotic treatment is required. A careful assessment of the pathogenicity of the organism, risks and benefits of therapy, the patient’s wish and ability to receive treatment as well as the goals of therapy should be discussed with patients prior to initiating treatment. In some instances, “watchful waiting” may be the preferred course of action.」
つまり、必ずしも診断即治療とはならないこと。菌の病原性の評価, 治療のリスクとベネフィット、患者の希望と、忍容性、また治療目標の設定を議論すること。そして「時には注意深い追跡が望ましい方針であるかもしれない」としています。
この後に、第一のPICOで治療すべき対象について記載している訳です。
これらを読んで、治療開始のタイミングを逸しないようにしたい、という意識が強くなった表現だと思いました。これまでは、主治医判断という面が強かったのですが、消極的なフォローアップによるデメリットが意識されたのだと予想しますし、予後解析の成果とも言えると思います。NBタイプは緩徐な進行を示しますが、空洞が形成(cavitary NB)されると治療反応性が悪くなることが明らとなっており、少なくとも診断時に空洞形成が確認されれば積極的な治療を考慮する必要がありますし、空洞が無くても塗抹などを参考に治療を検討する、と理解しました。
補足)NBタイプの進展による空洞形成はレントゲンのみでは判断が困難な時があります。
前回と同じ研究グループ(京都大学)が追加の検討を幾つか行っており、その一つを紹介します。
本研究では、MAC患者およびMAC感染のない人の土壌調査を行っています。その結果48.9%から同定され(農地7、庭79、鉢植え49)、その分離頻度は場所やMAC感染によって差異は無かったそうです。VNTRを行ったところ、M. avium(47の臨床分離株、41の土壌から分離)は78のパターンに分けられ、M. intracellulare(18の臨床分離株、37の土壌から分離)は53のパターンに分けられたそうです。臨床分離株と土壌でVNTRパターンが一致したのは6組あり、それは全て高暴露があるMAC患者であったため、土壌がMAC感染源の一つであると結論しています。

このグループ以外に、こんなにも綺麗にM. aviumとM. intracellulareを分離している研究は見たことがありません(凄い)。

前回の検討では週2回以上という表現でしたが、こちらは2時間で分けています。高暴露はM. avium、M. intracellulareに関わらず起こっているようです。
